The Effect of Large-Scale Anti-Contagion Policies on the COVID-19 Pandemic
Author Team: Solomon Hsiang, Daniel Allen, Sébastien Annan-Phan, Kendon Bell, Ian Bolliger, Trinetta Chong, Hannah Druckenmiller, Andrew Hultgren, Luna Yue Huang, Emma Krasovich, Peiley Lau, Jaecheol Lee, Esther Rolf, Jeanette Tseng, Tiffany Wu
All material below provided for free re-use with attribution to “Global Policy Laboratory, UC Berkeley. Source: Hsiang et al. (Nature, 2020)”
Table of Contents
Publication

Link to publication (Nature website)
Appendix
Detailed overview of how we acquired & processed the data used in this paper. (questions? → peiley@berkeley.edu)
Earlier versions (medrxiv.org)
Goldman School of Public Policy (GSPP) Feature about the team
Key Findings
In the absence of policy, we estimate that early infections of COVID-19 grow at a rate of roughly 38% per day. This implies a doubling time of approximately two days.
To evaluate the effect of anti-contagion policies, we collected information on 1,717 non-pharmaceutical interventions in six countries. The dataset includes policies deployed at both the national and sub-national (e.g. state, city) level.
Policies have different impacts on different populations. In general, we find that home isolation, business closures, and other large-scale social distancing measures have had large and measurable health benefits. We obtain mixed results for travel restrictions. We do not find strong evidence that some other policies, such as school closures, have significantly flattened the curve. See Figure 2 of the published article for more details.
We estimate that anti-contagion policies averted 62 million confirmed cases across the six countries in our sample (China, South Korea, Italy, Iran, France, and the United States) as of April 6, 2020. This corresponds to more than 500 million averted infections after accounting for under-reporting. See Figure 4 of the published article for more details, as well as country profiles at the end of this resource page (use buttons below).
China: 37 million confirmed cases (285 million total infections) averted as of 3/5/20.
South Korea: 11.5 million confirmed cases (38.5 million total infections) averted as of 4/6/20.
Italy: 2.1 million confirmed cases (49.4 million total infections) averted as of 4/6/20.
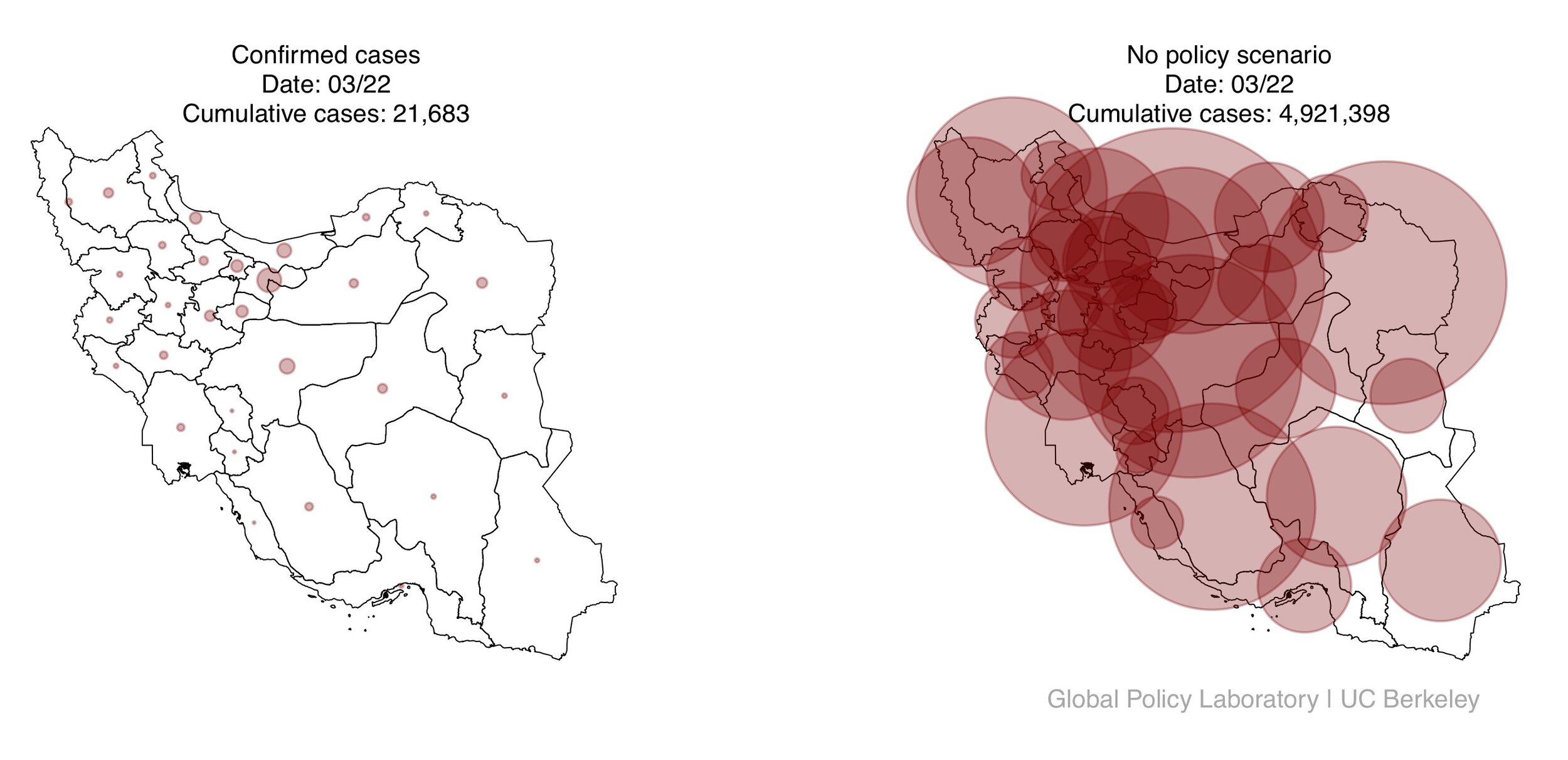
Iran: 4.9 million confirmed cases (53.8 million total infections) averted as of 3/22/20.
France: 280,000 confirmed cases (9 million total infections) averted as of 3/25/20.
United States: 4.8 million confirmed cases (59.9 total infections) averted as of 4/6/20.
Quick links to country profiles
Code and Data
Code and Data Repository
This Github contains the code and data necessary to replicate the findings of our paper on your own computing resources. (questions? → bolliger@berkeley.edu)
Code Ocean Capsule
This capsule contains the code used in our paper, as well as the environment in which to run it. It also provides access to a Stata license. (questions? → bolliger@berkeley.edu)
Data Dictionary
Describes the variables used in our analysis. (questions? → bolliger@berkeley.edu)
Data Sources
Epidemiological and policy information, as well as sources, for the 6 countries analyzed: China, France, Italy, Iran, South Korea, and the United States. (questions? → jeanette.tseng@berkeley.edu)
Contact Us About Data
If you have information regarding new data sources or would like to contribute data we missed, please let us know by filling out this form.
Data for Map Visualizations
To assist in creating data visualizations, we provide the number of confirmed COVID-19 cases by administrative unit (e.g. state) and date. We also provide our estimates for how many confirmed cases would have occurred in counterfactual world where no anti-contagion policies had been deployed. The data is provided in two formats, comma separated value (.csv) and shapefiles (.shp) for constructing maps.
Image Gallery























videos
Video recording of HELP Seminar presentation.
This seminar was presented to the Health and Pandemics Econo Working Group on May 1, 2020. The background, method, and concepts in presented are the same as in the final publication, however the numerical values presented are different because the data & analysis were updated between the seminar and the publication.
Country Profiles
China
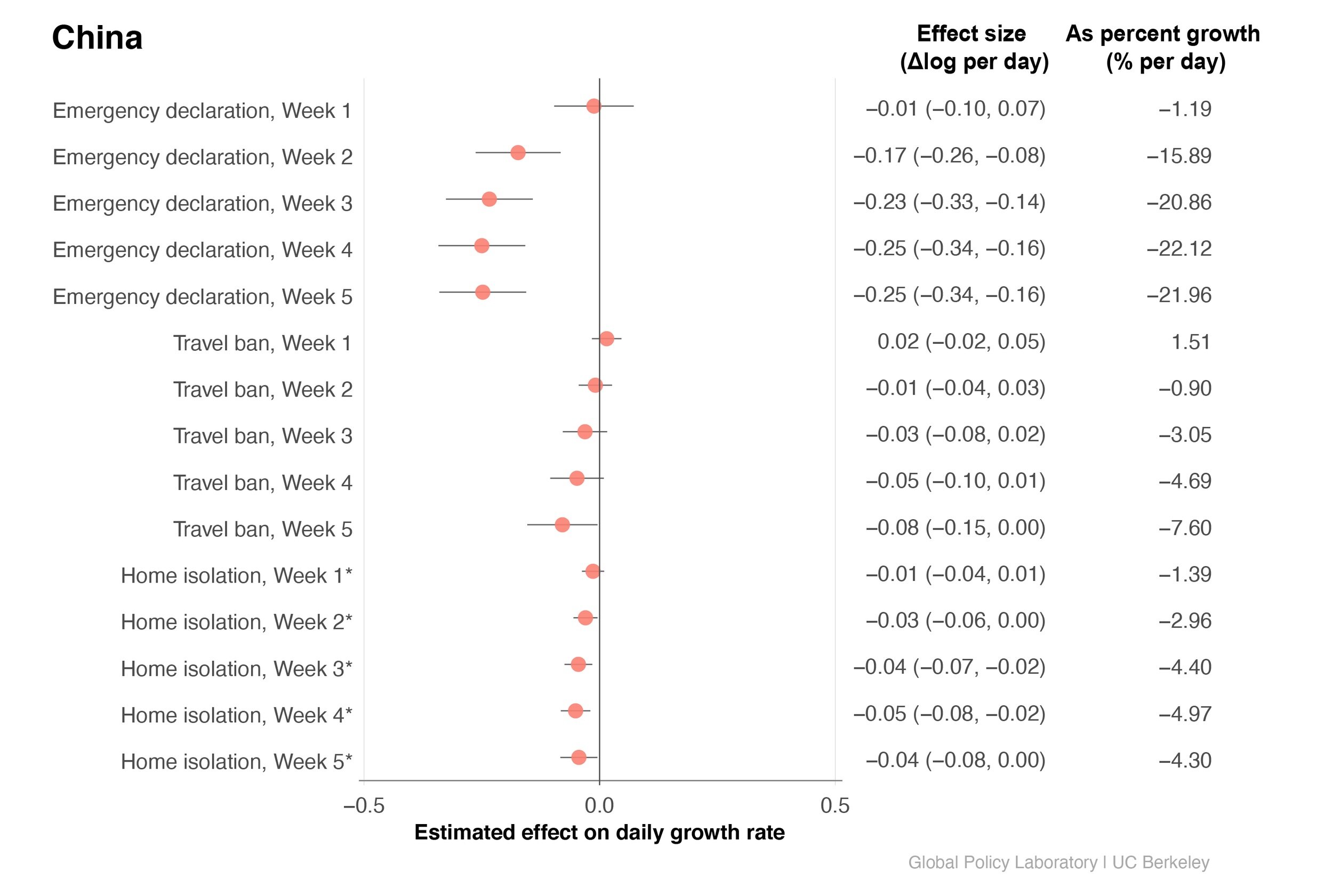
Area of circles show confirmed cumulative cases in 115 Chinese cities where data are available (shaded grey) daily between January 16 - March 5, 2020. Left: actual reported cases, right: estimated cases if no anti-contagion policies had been deployed.
在中国,我们研究了三个防疫措施:省级重大突发公共卫生事件一级响应(emergency declaration),封城(travel ban),以及小区封闭式管理(home isolation)。我们有以下几个主要发现:
在不采取任何公共政策的情况下,新冠肺炎感染人数的日增长率为36.21%,大约每两日翻倍。
三项政策均对遏制病毒传播有一定的作用,其中省级重大突发公共卫生事件一级响应的影响最为显著。
政策在第一周通常效果不显著,但从第二周起明显起效。
我们研究的三项政策共同减少了3700万的确诊病例(截止三月五日)。
中文媒体联络人:黄越
We study three anti-contagion policies: (provincial-level) emergency declaration, travel ban, and home isolation. Our main findings:
Without any policy intervention, COVID-19 infections grow by 36.21% per day, doubling roughly every two days.
All three policies have contributed to curbing the spread of the virus. Emergency declaration, a policy package deployed at the provincial level, is the most effective.
Policies tend to have small and insignificant effects in the first week, but have larger effects from the second week onwards.
The three policies we study averted or delayed 37 million confirmed cases in China (as of March 5).
For Chinese media inquiries, please contact Luna Yue Huang
See Appendix for more details.

South Korea
Area of circles show confirmed cumulative cases in South Korean provinces daily between February 17 - April 6, 2020. Left: actual reported cases, right: estimated cases if no anti-contagion policies had been deployed.
초기에 대한민국 정부는 우한시와 같은 코로나19 확산 지역으로부터 해외유입을 방지하는 데 주안점을 두었습니다. 그러나 2월 중순 신천지 교회와 연관된 확진자 수가 급증하게 되면서 코로나19 국내 확산을 차단하기 위해 전 국가적으로 한층 강화된 방역정책이 시행되었습니다. 우선 신천지 교회와 관련된 시설들이 폐쇄되었고, 사회 복지 시설들이 휴관되었으며, 검사 대상 범위가 늘어남과 동시에 시민 운집이 많은 도심에서 집회와 시위가 금지되기도 했습니다. 코로나19가 가장 급속하게 확산되었던 대구와 경상북도 일부 시군의 경우 피해 규모가 중대하여 특별재난지역으로 선포되었습니다.
본 연구에서 한국과 관련된 주요 내용은 다음과 같습니다.
적극적인 국내 방역 정책이 부재했을 때 코로나19의 성장률은 약 36.89% 이며, 이와 같은 성장세 하에서 코로나19 감염 건수는 2.2일마다 2배로 증가하게 됩니다.
만약 방역 정책이 실시되지 않았다면 높은 성장세로 인해 4월 6일에는 대한민국에 확진자 수가 약 11,500,000 명 더 존재했을 것으로 추정됩니다. 4월 6일 실제 국내 확진자 수는 9,924 명이었습니다.
한국에서는 신천지 교회 관련 시설을 폐쇄한 것이 가장 효과가 높은 정책 중 하나였던 것으로 나타났습니다.
기타 한국과 관련한 질문이나 언론 Contact 관련 문의사항의 경우 이재철 에게 연락 주시길 바랍니다.
Early interventions include the screening of travelers arriving from affected regions such as Wuhan, China. In February, the sudden rise in infections attributable to the Shincheonji Church resulted in the enactment of more aggressive policies nationwide, such as the closure of religious and welfare facilities, the prohibition of demonstrations and gatherings, and wider testing regimes. The regions hardest hit by the virus were largely due to the Shincheonji Church, including Daegu and its surrounding province, Gyeongsangbuk-do. These regions were designated as ‘Special Management Zones’.
Key takeaways:
In the absence of policy, the growth rate of COVID was 36.89%, or doubling every 2.2 days.
Without any policies, this growth rate would have led to about 11.5 million more cases by April 6th. In contrast, there were 9,924 confirmed cases on April 6th.
Policies with the highest impact include the closure of places of worship, particularly those related to the Shincheonji Church
For Korean media inquiries, please contact Lee Jaecheol
See Appendix for more details.




Italy
Area of circles show confirmed cumulative cases in Italian provinces daily between February 26 - April 6, 2020. Left: actual reported cases, right: estimated cases if no anti-contagion policies had been deployed.
Early policy interventions in Italy were implemented at the local level when municipalities and regions hard hit by the virus were placed under partial or full lockdown in late February/early March. Following these initial regional policies, nationwide policies were rolled out in quick succession, with all schools closed on March 5 and the entire nation being placed on lockdown five days later.
Key takeaways:
In the absence of policy, the growth rate of COVID was 45%, or doubling every 1.9 days.
Without any policies, this growth rate would have led to 2.1 million more cases by April 6th. In contrast, there were 132,547 confirmed cases on April 6th.
Policies that had the largest impacts were travel bans, suspending public transit through affected regions, and closing of businesses and schools.
See Appendix for more details.


Iran
Area of circles show confirmed cumulative cases in Iranian provinces daily between February 27 - March 22, 2020. Left: actual reported cases, right: estimated cases if no anti-contagion policies had been deployed
Early policy interventions in Iran were implemented in late February in the province of Qom, which was the initial epicenter of the outbreak. Policies were rolled out nationwide in early-mid March as the disease spread throughout the country.
Key takeaways:
In the absence of policy, the growth rate of COVID was 68%, or doubling every 1.3 days.
Without any policies, this growth rate would have led to 4.8 million more cases by April 6th. In contrast, there were 365,304 confirmed cases on April 6th.
The combined effect of an optional travel ban, closing of schools and a policing requiring that government employees work from home had the largest impact on slowing the spread of the disease.
See Appendix for more details.


France
Area of circles show confirmed cumulative cases in French regions daily between March 2 - March 25, 2020. Left: actual reported cases, right: estimated cases if no anti-contagion policies had been deployed.
Les politiques publiques en France ont en grande partie été coordonnées au niveau national, bien que plusieurs mesures furent prise plus localement. Trois des restrictions les plus importantes - fermeture nationale des écoles et universités, fermeture des commerces non-essentiels et confinement de la population - ont été proclamées dans un laps de temps particulièrement rapproché. Il est donc difficile de détecter séparément leur impact, à l’exception des fermetures d’écoles dont certaines ont eu lieu avant le décret national.
Les points clefs de notre étude:
Le taux de croissance journalier du nombre d’infectés en l’absence de politique publiques est de 38.96%, soit un doublement du nombre de cas tout les 2,1 jours.
Sans interventions, un tel taux de croissance aurait porté le nombre de cas confirmés à 304000 à la fin de notre échantillon le 25 mars.
L’interdiction précoce des grands rassemblements a eut un impact déterminant.
La fermeture des commerces et le confinement de la population ont conjointement contribué à freiner l’épidémie.
Pour toutes informations supplémentaires, veuillez contacter Sébastien Annan-Phan
Interventions in France were primarily coordinated at the national level, even though several measures were enacted locally. Three out of the four most important policies - school closure, business closure and the shelter in place - were enacted within a short time interval. It is thus challenging to isolate their separate effects, except for the effect of school closure since we observed some closing of regional schools prior to the national policy closing all schools.
Key takeaways:
The infection growth rate in the absence of intervention is 39%, or a doubling of cases every 2.1 days.
Without policies, we estimate there would have been 304,000 confirmed cases in France by the end of our sample on March 25.
The early no gathering and social distancing policies had a large effect. Business closure and shelter-in-place also contributed to slowing the epidemic.
For press inquires, please contact Sébastien Annan-Phan.
See Appendix for more details.


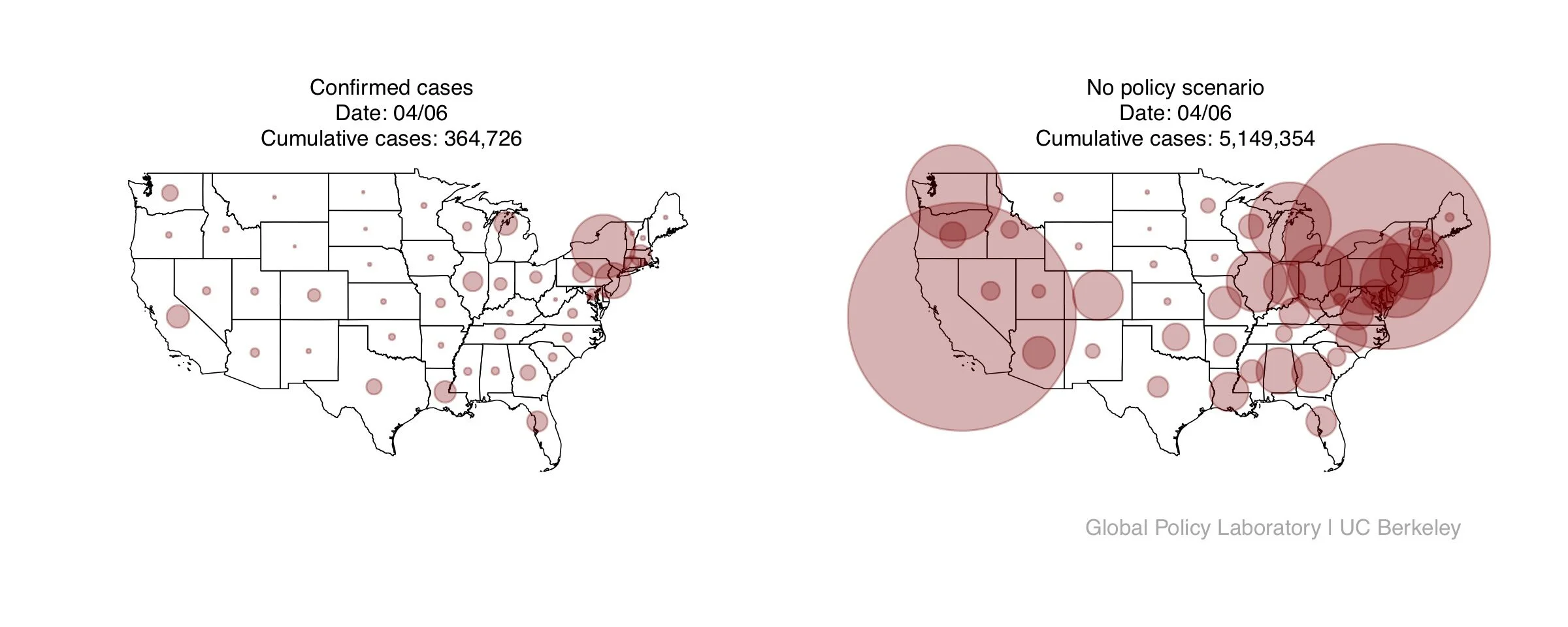
United States
Area of circles show confirmed cumulative cases in US states daily between March 3 - April 6, 2020. Left: actual reported cases, right: estimated cases if no anti-contagion policies had been deployed.
Most policies in the US were implemented at the state or local level, with localities differing on the types of policies enacted and when the policies were implemented. States that were affected by the virus early on, such as Washington, California and New York, were one of the first jurisdictions to enact policies starting in early to mid-March. Additionally, the federal government issued a "15 Days to Slow the Spread" social distancing guidelines on March 16. All states had implemented some forms of policy by the end of our sample period.
Key takeaways:
In the absence of policy, the growth rate of COVID was 34%, or doubling every 2.4 days.
Without any policies, this growth rate would have led to 4.8 million more cases by April 6th. In contrast, there were 365,304 confirmed cases on April 6th.
Policies that had the largest impacts were social distancing policies, shelter-in-place, closing businesses, and quarantining of positive cases.
See Appendix for more details.


Frequently Asked Questions
Q. What is your study about?
Our study evaluates the efficacy of anti-contagion policies designed to slow the spread of COVID-19. While the economic and social costs of these policies are highly visible the health benefits, in the form of infections and deaths that would have occurred but are instead avoided or delayed, are unseen..
We find that in the absence of policy intervention, the number of COVID-19 infections was doubling approximately every two days. This finding is consistent across all studies in our sample, except for Iran, which exhibits even faster growth.
We document that federal and local governments in the six countries we study deployed more than 1,700 anti-contagion policies implemented between January and April 2020.
These policies have substantially flattened the curve. We estimate that, together, these policies averted of 62 million confirmed cases, and 530 million total infections (accounting for under-detection) as of the beginning of April in the six countries we study (China, South Korea, Iran, Italy, France and the United States).
In contrast, the total number of confirmed cases across these six countries through the end of our sample time period is 1.6 million cases, or about 2.6% of the counterfactual 62 million cases.
Q. What countries did you study, and why?
We analyzed the impact of policies on the spread of COVID-19 in China, South Korea, Iran, Italy, France, and the United States. It was our hope to learn from the recent experience of these six countries, where early spread of the virus triggered large-scale policy actions.
Q. What policies did you analyze?
We analyzed the full set of policies that were implemented in each of the six countries. We collected subnational data, so we were able to account for policies that were implemented at the city, state or province level, as well as at the national level.
While the actual details of each policy varied across localities, the policies we analyzed fall into four main categories:
Restricting travel
Distancing through the cancellation of events and suspension of educational/commercial/religious activities
Quarantine and home isolation
Miscellaneous policies (including providing paid sick leave and declaring a state of emergency)
See Appendix for more details on policies.
Q. What are included in these policies and how do they differ by country?
Here are some of the more salient policies by country:
China:
Emergency declarations include closing of entertainment venues, banning of public gatherings, and extensive temperature monitoring at airports, railway stations and highway checkpoints.
Travel bans include banning any local travel into or out of the city.
Home isolation policies are lockdown policies where school and businesses are closed, and residents are placed under household quarantine.
Korea:
Other social distance policies include recommended policies to minimizing gatherings.
Italy:
The home isolation policy constitutes a lockdown policy.
The other social distance policies include maintaining one meter distance from others in public.
Iran:
The work from home policy mandates that government employees must work from home.
France:
The combined business closure and home isolation policies constitute the national lockdown.
The cancel events, no gathering, and other social distance policy package includes banning audiences at professional sport events, prohibiting gatherings of a certain size, and limiting visits to long-term care facilities.
US:
Home isolation policies include shelter-in-place policies and all of the policies enacted alongside shelter-in-place, including work from home, business closures, and no gathering policies.
“Slow the spread” guidelines are the federal social distancing guidelines issued on March 16, 2020.
For additional policy information, please see the “Chronology of Policy Implementation” and the “Policy Data” Overview sections in our Supplementary Information.
Q. What policies are included in the “other social distancing” policy category in the US?
This policy category includes a wide range of mandatory and optional guidelines that aimed to keep people physically distant from one another. This includes:
Isolate certain populations: recommend or mandate the isolation of populations such as the elderly, immunocompromised or those who have recently returned from a cruise
If outside the home, must abide by social distancing standards: require a six foot minimum distance from others outside the home, maintain distance when riding public transportation, ask that businesses restrict the number of people within storefront at a time as well as restricting certain types of activities that involve physical interaction with customers (e.g., bagging groceries, taking cash payment)
Mandate mask wearing: require people to wear a mask outside the home
Close public facilities: close libraries, museums, flea markets, historic sites, memorials, and polling locations
Close outdoor facilities: close beaches, state parks, public parks, public toilets, lakes, and campgrounds.
Social distance restriction of visitation to certain facilities: restrict visitation to prisons, long term care facilities, child care facilities, and homeless shelters, stop elective medical and veterinary procedures, and bar short term rental accommodations.
Suspend non-critical state operations/government services: close government buildings, stop in person meetings of people working for the state, suspend court operations, waive or extend licensing, and permit certain types of work to be carried out remotely, when normally could not (e.g., notaries, police work, licensing)
Q. Which policies do you find worked best? Which policies didn’t work as well?
We find that while the overall combined effect of policies substantially reduced the spread of COVID-19 in each of the six countries, the individual policies that worked best differed by country. Given that policy details and implementation varied substantially across jurisdictions, and the populations across our six countries are very different, it is important to assess the effectiveness of policies by country.
We find that home isolation (“lockdown” or “shelter-in-place”), business closures, and large scale social distancing policies, have big effects.
The effect of the travel ban is mixed, and we don’t find strong evidence of school closures having significantly flattening the curve.
Q. What will happen if we lift these policies?
Our study looks specifically at the implementation of policy. We don’t have sufficient data to evaluate how the lifting of policies would affect the spread of the coronavirus. One piece of evidence that might shed some light are our results from China, where we had enough data to evaluate how the effects of policies evolved over time. We find that the largest effects of the policy on depressing the spread of the virus are realized several weeks after deployment. This suggests that if we were to lift these policies, it would not be unreasonable to expect a similar two to three week delay before we see a marked increase in cases.
It is likely that the growth rate of COVID-19 infections will not reach the levels seen before the policies were deployed because society's awareness of the virus has changed remarkably since the first wave of infections.
Q. Do you account for underreporting and changes in testing?
Yes, we account for both underreporting and changes in testing. We used an econometric approach that allows us to examine the impact of policies on growth rates without having to make an assumption about what the percent of cases go undetected. Furthermore, we compile a dataset on changes in testing regimes and case definitions by country so that we can account for these changes.
Q. Why do the sample end dates differ across countries?
For most of the countries in our sample, our data go through April 6, 2020. However, in Iran, our sample period ends on March 22, and in France, on March 25, because the governments stop releasing subnational case data. In China, our sample period ends on March 5 since cities begin lifting lockdown policies after that date.
Q. What can you say about how many deaths have been averted?
We do not analyze data on deaths. Since we estimate that millions more infections would have occurred if no policies had been deployed, we cannot assume the infection fatality rates estimated in the scientific literature would still hold in a scenario where the health care system was overwhelmed to such an extent.